Primary teeth, baby teeth, milk teeth, deciduous teeth, temporary teeth…
There are many names for your baby’s first teeth. While primary teeth development most often follows a certain sequence, variations can happen, and it is good to be aware of whether the development you see in your child is normal or something that a dentist or pediatrician should address.
In this article, we go through normal and abnormal teeth development and answer common questions parents have about their young children’s teeth.

In this Article:
When Do a Baby’s Teeth Develop?
Tooth development occurs before birth. It begins with the formation of a “bud” within the fetal gum tissue at six weeks gestation. A central area of this tissue thickens to form what is called a tooth “bud”, which continues to grow into a structure that will become the center of a new tooth. The middle and outer tooth layers grow around this central area at 12 to 16 weeks gestation.
The Anatomy of a Tooth
A tooth consists of four layers: enamel, dentin, pulp, and root. Teeth are situated within the gums of the upper jaw (maxilla) and lower jaw (mandible).
Enamel
This is the outermost tooth layer, visible as a hard, white covering. Enamel is the hardest substance in the human body.
Dentin
This layer lies just beneath the enamel and surrounds the pulp. It is the majority of a tooth’s structure.
Pulp
This central portion of a tooth houses the nerves and blood vessels. It also contains the components needed for the dentin layer. When tooth pain develops, it originates from the pulp.
root
The root is the pointed section of the tooth, imbedded into the gums. It secures the tooth to the jaw bone. The front teeth have one root, while larger teeth may have two or three roots.
Calcium and phosphorus are the minerals necessary for forming enamel and dentin. Without enough calcium during teeth development, magnesium and sodium become the primary components, resulting in less durable teeth.
Normal Primary Teeth Eruption
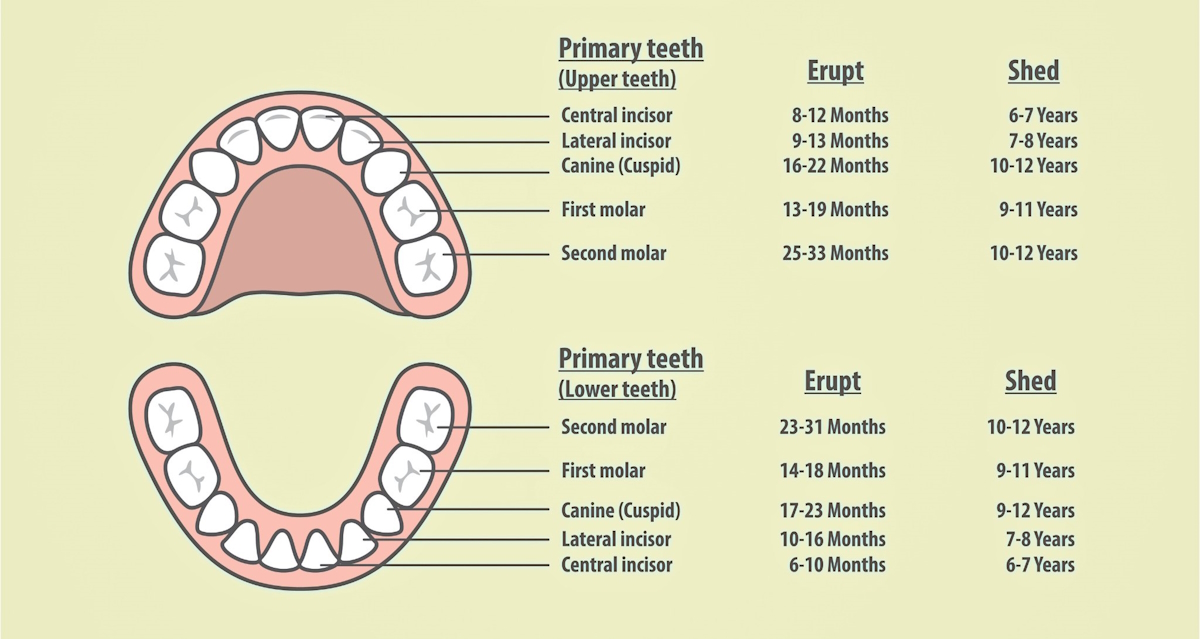
The above chart of the primary teeth shows both normal baby teeth eruption and shedding.
For most infants, the first tooth appears between ages six to 12 months. Before this, there may be signs of teething, such as increased drooling or gnawing on fingers and objects. Discomfort from the pressure of the erupting tooth against the gums is common. Infants may seem particularly uncomfortable when molars or more than one tooth erupts at once.
Primary teeth usually erupt in a specific sequence: incisors first, then the first set of molars, then the cuspids, and then finally the second set of molars.
incisors
The front upper and lower teeth are known as incisors. They are used to bite into foods, but infants may use them to chew before other teeth erupt. The incisors are usually the first teeth to appear.
| Incisors Eruption Order | Child’s Age |
|---|---|
| Middle lower incisors | 6-10 months |
| Middle upper incisors | 8-12 months |
| Lateral lower incisors | 10-16 months |
| Lateral upper incisors | 9-13 months |
Cuspids
These are also called the “canine” teeth because of their pointedness. Cuspids are located lateral to the incisors and usually erupt after the first molars.
| Cuspids Eruption Order | Child’s Age |
|---|---|
| Lower cuspids | 17-23 months |
| Upper cuspids | 16-22 months |
Molars
The molars are the larger teeth in the back of the mouth that are important for chewing foods. The first set typically erupts after the incisors. The second molars are the final primary teeth to erupt, usually after the second birthday.
| Molars Eruption Order | Child’s Age |
|---|---|
| First lower molars | 14-18 months |
| First upper molars | 13-19 months |
| Second lower molars | 23-31 months |
| Second upper molars | 25-33 months |
Several months may pass between the appearance of the cuspids and second molars. Your toddlers (and we, parents) get a much-needed break from the discomfort of teething during this phase. If a two-year-old suddenly develops crankiness and begins to drool again, it is likely that the second molars will soon erupt.
Ultimately, there should be a total of 20 primary teeth.
Abnormalities in Tooth Eruption
Natal and Neonatal Teeth
Can babies be born with teeth?
Yes, there are rare occasions where one or more teeth are present already at birth. In other cases, neonatal teeth erupt within the first 30 days of life. Although the exact cause is unknown, such early teeth eruption is thought to be the result of some sort of prenatal stress.
Most natal or neonatal teeth are the lower incisors. They can cause trauma to the infant’s tongue while feeding and cause pain for breastfeeding mothers.
These early teeth may be an isolated finding or one of many features of a genetic syndrome. If they become loose, they are an aspiration risk. Unless this is a concern or an infant cannot feed, extraction is generally not recommended.
Congenitally Absent Teeth
There are times when primary teeth fail to develop during fetal life. This becomes apparent when some teeth are missing, as others erupt.
The absence of primary teeth may be due to genetics; a parent may have had the same issue as an infant. Missing teeth are often associated with chromosomal abnormalities such as Down syndrome and others. Prenatal exposure to maternal infections, illnesses, or certain medications may also be the cause.
Whether or not intervention is necessary depends on the number of missing teeth and its effect on the child’s quality of life. If many teeth are absent, partial dentures may be recommended if age-appropriate.
Delayed Tooth Eruption
Worrying that your baby has no teeth yet is common among parents. However, the timing of tooth eruption can vary by gender, race, and ethnicity. If there are no teeth by the first birthday or all 20 teeth have not appeared by age four, this warrants an evaluation by a dentist.
There are various reasons why some teeth may take longer to erupt than others:
Gum/Gingiva Problems
If there is an abnormality on the surface of the gums, this can impede tooth eruption. Thickened gums due to prenatal exposure to certain medications or maternal vitamin C deficiency can block the path of tooth eruption.
If there is a tumor, scar tissue, or other defect, this can create a barrier. However, a blood vessel that overlies an erupting tooth should not cause interference. As the tooth pushes past this blood vessel, there may be a small amount of bleeding under the gums, noted as a bluish discoloration. This phenomenon is normal and typically does not affect the tooth itself or the timing of its eruption.
Problems with Tooth Development
If the inner tooth dentin fuses to the jaw bone during fetal development, that tooth cannot erupt.
Prematurity and Low Birth Weight
Infants born before 30 weeks gestation and/or with a birth weight below 1000g are at risk for delayed tooth maturation and eruption. Infants who are small for gestational age or don’t grow sufficiently in utero are also at risk.
Nutritional Factors
Delayed tooth eruption may occur if an infant does not receive sufficient nutrients via the placenta or after birth. The incidence is higher in communities where access to nutritious foods is limited. Breastfeeding is thought to be preventative.
Medical Conditions
In addition to genetic syndromes, some infant and childhood medical conditions can delay teeth eruption. These include congenital HIV infection, hypothyroidism, pituitary dysfunction, cerebral palsy, anemia, and kidney disease.
Disorders Associated with Abnormal Tooth Shapes or Colors
Several medical conditions noted at birth can result in abnormal primary teeth. They may be associated with other physical abnormalities, so early detection is important. Some of these children require multidisciplinary care throughout their lives.
Congenital Syphilis
Over 130,000 cases of syphilis were reported in the U.S. in 2020, and the numbers continue to increase. Syphilis is a sexually acquired infection that can be transmitted to a fetus via the placenta.
Among other facial abnormalities, syphilis can impair fetal tooth development, resulting in Hutchinson Teeth. When teeth erupt, they are narrow and have notches.
Amelogenesis Imperfecta
The enamel fails to form properly in infants with amelogenesis imperfecta. Because of insufficient calcium and phosphorus within the enamel, teeth have a yellow or brown discoloration.
This condition may be the result of an infection, vitamin D deficiency during pregnancy, or a genetic mutation.
Once erupted, the teeth are fragile, crack frequently, and are prone to decay. In addition to cosmetic challenges, there may be sensitivities to temperature and certain foods.
Ectodermal Dysplasia
Ectodermal dysplasia can be inherited from a parent or due to a genetic mutation. It is characterized by poorly developed hair, skin, teeth, and nails.
Teeth are small, globe-shaped, or widely spaced. Some primary teeth may be absent. Development of tooth enamel is also affected, which increases the risk of tooth decay.
Tetracycline Teeth
Prenatal exposure to tetracycline and similar antibiotics can cause staining of fetal teeth. These antibiotics are used to treat illnesses such as Lyme disease, sexually transmitted infections, and resistant Staphylococcus (MRSA). The medication accumulates within the “tooth bud,” and binds to calcium, forming dark-colored areas within the dentin and enamel.
Exposure to Chemotherapy
Pregnant mothers undergoing cancer treatment with certain chemotherapeutic drugs may have infants with discolored teeth. If treatment is initiated during the first trimester, the size of the primary teeth may be smaller than expected.
Hyperbilirubinemia
Jaundice, a yellow coloring of an infant’s skin, is common during the first week of life. It is caused by the blood pigment bilirubin deposition into the skin and eyes. If noted during the first few days of life, the bilirubin level is checked at the hospital. Bilirubin levels above 15 require intervention to prevent further elevation that could harm an infant’s brain.
High bilirubin levels are also associated with a green discoloration of teeth. This is due to bilirubin deposition into the dentin.
Keeping Infant and Toddler Teeth Healthy

Although sometimes not prioritized, oral care is important to infant and toddler health. Even before teeth erupt, parents should gently clean their baby’s tongue with a moist washcloth to decrease milk accumulation and wipe the gums once pureed foods are introduced.
After the first teeth erupt, parents should begin to brush them at bedtime. Incisors may be easily cleaned with an over-the-finger type of toothbrush, but a handle-type one is appropriate once molars erupt.
Fluoride
Fluoride helps to harden tooth enamel and is very important for cavity prevention. Although there are many fluoride-free toothpastes available on the market, both the American Dental Association and the American Academy of Pediatrics recommend fluoride toothpaste for all ages:
| Age | Amount of toothpaste |
|---|---|
| Ages 6 months to 3 years | “grain of rice”-sized smear of toothpaste |
| Ages 3 years and up | “pea-sized” amount of toothpaste |
Children over age two can be taught to spit out the toothpaste. These fluoride recommendations are based on increasing rates of cavities and poor oral health among children.
For communities without local water fluoridation, prescription fluoride supplements are recommended. These are taken daily and are dosed based on age:
| Age | Fluoride supplement amount |
|---|---|
| Ages 6 months to 3 years | 0.25mg fluoride/mL |
| Ages 3 to 6 years | 0.5mg fluoride/mL or tablets |
| Ages 6 and up | 1mg fluoride tablets |
Parents should contact their municipality to determine if fluoride is included in their local water treatment process.
Dental Visits
The American Dental Association recommends that infants see a dentist after the first tooth erupts between ages six to 12 months. This is not a visit for a dental cleaning but to assess for potential problems. For example, some infants are born with a prominent connective tissue between the upper lip and central incisors. This can make it difficult to keep the upper teeth clean and increase the risk of dental caries.
Routine dental visits are recommended every six months. Once all teeth have erupted, dental cleanings may begin.
Aside from routine care, parents should take their baby to a dentist if the teeth appear abnormal upon eruption. A dental evaluation should be part of the care plan if an infant is born with a medical condition that can affect the teeth.
If no teeth have erupted by 13 months, or some teeth are still missing at age four, further evaluation is necessary.
Parents’ Common Questions About Primary Teeth Development
My baby’s teeth are “coming in crooked.” What should I do?
It is not unusual for an infant to have a few teeth that are misaligned. This is often due to family history. Most cases are not associated with secondary teeth problems or misalignment.
The baby should see a dentist if misaligned teeth cause cheek or lip trauma while eating.
Why are my baby’s top front teeth not coming in? Is it normal for teeth to come in out of order?
Some infant teeth deviate from the usual eruption order, for example, getting the lateral incisors before the central ones. In most cases, this is not a cause for concern. However, parents should speak to a dentist if the central teeth fail to erupt after a few months while others appear.
My baby’s teeth look malformed. What should I do?
If your baby’s teeth seem abnormal in shape, size, or color, you should speak to your pediatrician and dentist. Some tooth disorders are associated with other medical problems that need to be addressed. Your baby’s dentist can explain why the abnormalities have occurred and what can be done.
Why does my baby have mottled teeth, and what should I do?
“Mottled” is a general description for teeth that have white, yellow, or brown spots, sometimes with a defective surface. There are several reasons that teeth may develop mottling, so you should discuss this with a dentist.
One possible cause is the ingestion of too much fluoride. This commonly occurs when excessive fluoride is present in drinking water. No more than 0.07mg/kg of fluoride should be ingested daily to prevent tooth fluorosis. Parents should be aware of the fluoride content in their local water sources.
Is it normal for a 12 to 15-month-old to have no teeth?
At 12 months, some toddlers are just getting their first two teeth, which is relatively late but still within the normal range.
However, suppose there is no sign of impending eruption (swollen gums with underlying teeth imprints). In that case, the toddler should be evaluated for possible missing teeth or a gum problem. 13 to 15-month-olds without teeth also need further evaluation.
Takeaway
In most cases, a baby’s primary teeth development will follow the expected route, and the teeth that erupt will be healthy and look normal. In this case, the only things we parents have to do are to ensure careful teeth care and help our children with their teething pain.
However, it is important to be aware of the abnormal primary teeth development that can occur and consult a pediatric dentist with any worries.
Read Next
- 5 Effective Teething Remedies to Mitigate Your Baby’s Pain
- Is Your Baby Teething? 11 Infant Teething Symptoms to Know!
- My Baby Has No Teeth?! Late Tooth Eruption: A Worry or Not?
- My 3 Month Baby Is Crying And Sucking His Hand – Teething, Hungry or What?
- 5 Toddler & Baby Teeth Care Tips for Cavity-Free Baby Teeth
Research References
- John Hopkins Medicine:The anatomy and development of the mouth and teeth
- Morris AL, Tadi P. Anatomy, Head and Neck, Teeth. [Updated 2023 Jul 24]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-.
- Srđan Nedoklan, Zlatka Knezovic, Nina Knezovic, Davorka Sutlovic, NUTRITION AND MINERAL CONTENT IN HUMAN TEETH THROUGH THE CENTURIES, Archives of Oral Biology, Volume 124, 2021.
- Newadkar, Ujwala Rohan1,; Chaudhari, Lalit1; Khalekar, Yogita K.1. Natal and neonatal teeth: Terminologies with diverse superstitions!!. Journal of Family Medicine and Primary Care 5(1):p 184-185, Jan–Mar 2016. | DOI: 10.4103/2249-4863.184663

Paula Dennholt founded Easy Baby Life in 2006 and has been a passionate parenting and pregnancy writer since then. Her parenting approach and writing are based on studies in cognitive-behavioral models and therapy for children and her experience as a mother and stepmother. Life as a parent has convinced her of how crucial it is to put relationships before rules. She strongly believes in positive parenting and a science-based approach.
Paula cooperates with a team of pediatricians who assist in reviewing and writing articles.




